Identifying area for improvement
The first challenge on your improvement journey is to identify whether there are areas of the care you provide for frail older patients that could be improved. This closely associates with a second challenge – convincing others that the solution to the problem is the right one.
You will start defining the problem in your service which can be improved by introducing the process of holistic assessment and co-ordination of frail older patients known as Comprehensive Geriatric Assessment (CGA – see Box 2). CGA is the accepted gold standard method of care for frail older people in hospital.
|
CGA is defined as ‘a multidimensional, interdisciplinary diagnostic process to determine the medical, psychological, and functional capabilities of a frail older person in order to develop a coordinated and integrated plan for treatment and long-term follow-up’ (14). |
To demonstrate the value of the introduction of Comprehensive Geriatric Assessment (CGA) into your systems and processes, it is vital to be able to show how it has made a difference to the quality and effectiveness of the service provided. There is good evidence from the international research literature that introducing CGA is associated with improved outcomes at various levels, including service-level outcomes reduced length of stay and reduced in-hospital complications, and potential system-level cost savings. The following table summarises the evidence found in a recent review of reviews of CGA interventions:
| Outcome | Metric | Effec Size | Cost Savings? | Review References |
| Length of stay |
Length of stay at discharge |
Mixed – ranging from no significant difference to significant difference (p=0.02), and trend to reduction in length of stay from 4-9 days over the reviews | Reduction in costs1; suggests optimal for overall outcome achievement7; slightly, significantly lower cost of hospital care11 | Ellis et al.1*, Fox et al.2*, van Kraen et al.3, Kammerlander et al.4, Fox et al.7*, Deschodt et al.9, Ellis et al.10*, Baztan et al.11, Fealy et al.12 |
| Readmissions | Readmission to hospital at one month, three months, six months and one year | No significant effects in most reviews. Negative effect in one study. Trend of 15% less likely to be readmitted | Ellis et al.1*, Fox et al.2, van Kraen et al.3, Linertová et al.5, Conroy et al.6, Deschodt et al.9, Ellis et al.10*, Baztan et al.11, Fealy et al.12 | |
| Admission to long term care |
Discharged to and living at home Institutionalisation (living in residential care at end of scheduled follow-up |
Between 5 and 30%
All reviews except 11 showed meaningful trend up to significant reduction in admission to care |
Ellis et al.1*, Fox et al.2*, Fox et al.7*, Ellis et al.10*, Bazta et al.11
Ellis et al.1*, Fox et al.2*, van Kraen et al.3, Conroy et al.6, Fox et al.7*, Ellis et al.10*, Baztan et al.11, Fealy et al.12 |
|
| Other service level outcomes |
Cost of Geriatric Unit Overall Societal costs |
p=0.02 No quantitative analysis |
Costs of acute unit care were significantly lower than usual care Each study reported was ‘cost effective’ in not increasing overall societal cost CGA may lead to a small increase in costs, and evidence for cost-effectiveness is of low-certainty due to imprecision and inconsistency among studies. |
Fox et al.2
Fox et al.7
Ellis et al.1* |
| *Reference 1 reviewed the same studies as reference 10; Reference 2 reviewed the same studies as reference 7 | ||||
Impact of CGA Studies
Some studies have looked at the impact of CGA on the process of care and reduction in complications that in turn, lead to the service related benefits, such as reduced length of stay. For example, the ‘POPS’ evaluation has shown that the intervention group had fewer post-operative medical complications including pneumonia (20% vs 4% [p = 0.008]) and delirium (19% vs 6% [p = 0.036]), and significant improvements in areas reflecting multidisciplinary practice including pressure sores (19% vs 4% [p = 0.028]), poor pain control (30% vs 2% [p<0.001]), delayed mobilisation (28% vs 9% [p = 0.012]) and inappropriate catheter use (20% vs 7% [p = 0.046]). Length of stay was reduced by 4.5 days. There were fewer delayed discharges relating to medical complications (37% vs 13%) or waits for OT assessment or equipment (20% vs 4%). (15,16,9)
Services that have successfully improved care for frail older patients demonstrated how introducing holistic assessment and management for frail older patients was also about “making life easier” for the service. Identifying the right problem was key.
You may therefore wish to target improvements in one of these outcomes through your efforts to improve your service. Establishing a local baseline for these outcomes will be one of your first steps.
Convincingly demonstrating an impact on ‘distal’ outcomes, such as length of stay or quality of care is more difficult in day-to-day service provision than in research settings, where numbers of patients are smaller, patient characteristics are more varied, and resources for measurement across the patient pathway are more constrained. Therefore it may be better to be more modest in what you measure, focusing for example on process measures rather than service outcomes, making good use of routinely collected and readily available data, and ensuring any additional data collection is feasible and carefully targeted.
As well as being important in demonstrating the value of change to others, measurement is also crucial for understanding and evaluating the impact of change within your team. Chapter 5 of the How to Improve guide produced by the Welsh 1000 Lives Plus campaign contains useful guidance on measurement for improvement. Effective measurement for improvement is about getting the right balance between the burden of extra data collection and interpretation, which can be time-consuming, and ensuring that you have collected enough data, consistently, to be able to understand the impact your changes are making. Run charts are a simple, but statistically robust, way of plotting how measures are, or are not, changing over time, and whether or not the changes you are making are resulting in real and sustained shifts in the processes and outcomes intended.
Using data to define the problem and to monitor it continuously throughout your journey will allow you to:
- know where your service stands in relation to the standards of care
- generate interest in those in charge of finance
- generate buy-in from colleagues
- identify what is working well and what is not working so well in improving care
- ultimately, show the benefits of improvement
This data is different from data for judgment; the latter is not helpful in developing a service. It is important that you negotiate the use of measurement for improvement with those overseeing the evaluation of the service so that they do not rush to judge a service before it is ready for judgement! It may take many months to establish a service to stage where a more summative assessment can be undertaken to look at the relative benefits.
In considering whether your service can provide better care for frail older patients you may also wish to look at:
- web-based ‘frailty dashboard’ indicating the size and nature of the problem derived from the Nuffield data [CS(1] – this will look at service level outcomes, such as attendance and admission rates, bed-days (not length of stay as this is very dependent upon admission rates), readmission rates. You may also be able to collate some patient related outcomes, such as satisfaction (e.g. friends and family test), and mortality. Other patient related outcomes such as function, mood, quality of life are fantastic if available but not routinely collected as outcomes in most places.
- national reports from Royal Colleges
- data from the NHS benchmarking audit on acute care for older people[1]
- patient stories[2]
These data sources can be useful for working out the nature and size of the problem, and therefore what to focus on improving – in contrast to process measures that should be used during the improvement process itself.
[CS(1]Link to Nuffield toolkit
Using data for improvement
Below is an example of the use of data for improvement – in this case establishing a process to identify frailty in the emergency department – but the principles apply other areas too:
Making the use of frailty tools part of an everyday practice takes a bit of time, but it is not that difficult. There are four key steps, each of which is a PDSA cycle.
- The ambulance service will almost certainly be able to provide the information necessary to use one of the frailty tools. This admission interface covers that vast majority of patients relevant to frailty services.
- When the ED or AMU nurse takes a handover from the ambulance service, they need to populate a frailty box on the handover proforma that all hospitals will use. Different versions can be found in different hospitals, but all hospitals have some sort of handover/immediate assessment form.
- This frailty score can then be added to your electronic hospital record. Different systems operate in different hospitals, some covering just ED, some also including the AMU and the rest of the hospital. If your setting is IT ready, then ask your IT team to create a frailty field, which can be used for tracking purposes.
- The final step is to check that the frailty identification leads to an action. Depending on your setting, this might be a referral to a frailty team, frailty unit, or special documentation – however your deliver CGA, check that it is being done for older people with frailty and urgent care needs.
Embedding frailty tools in your setting will be greatly aided by the use of PDSA cycles.
Step 1 check that the ambulance crew provide most of the information required
For this you will need a clinical data collector – nurse specialist, doctor, therapist, whoever, just so long as they know what the information means and can turn it into your chosen frailty score. Check the process works using run charts – remember, you don’t need to check many patients – perhaps just ten older patients (65+) should be enough. You’ll then get a run chart that looks something like this where 1 means that patient could be scored and 0 means they could not:
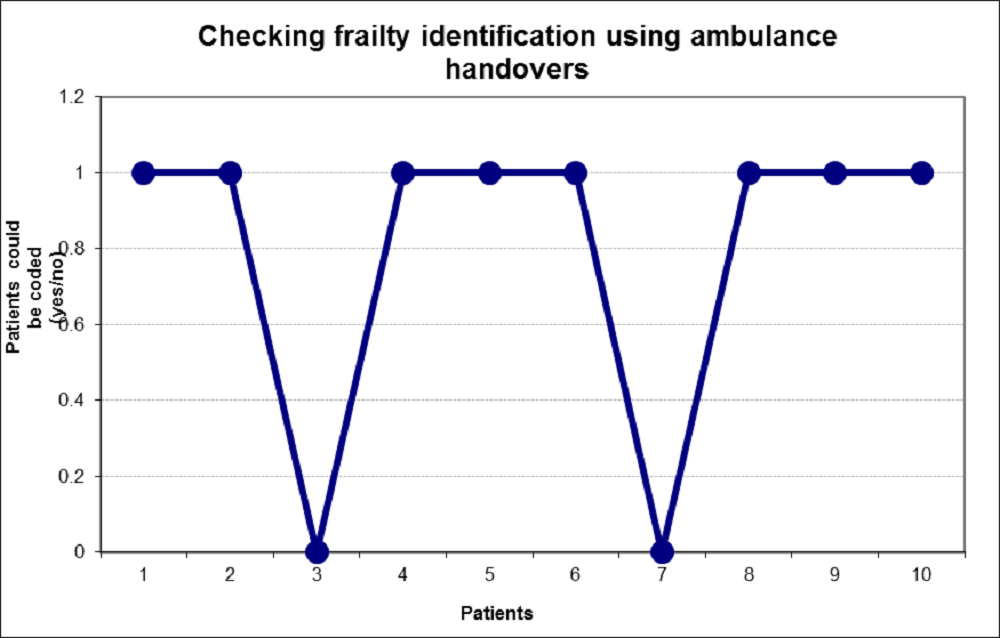
This one shows that two patients could not be coded – you need to understand why not, and if appropriate change the process to ensure that they can be coded in the future. It might be that the ambulance service are not capturing information on cognition, in which case you need to get them to start doing so. It might take a while to sort, but if the ambulance team scan see how this will help their patient, and reduce their waits in ED, then they will be happy to help. You might need to get some senior support.
Test again after the process change and you will hopefully get a run chart like this:
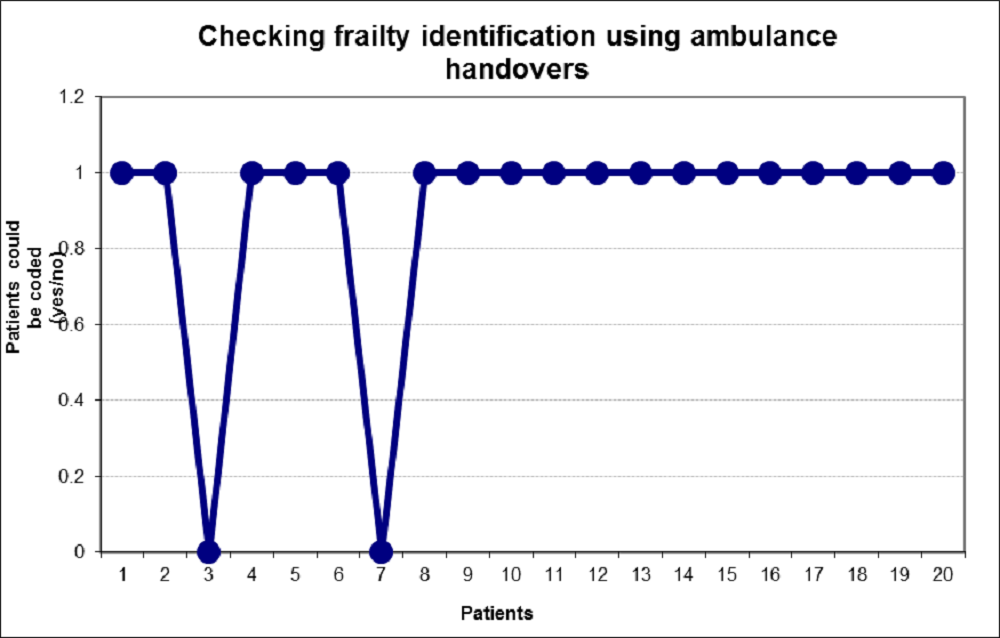
As you will know by now, a run of eight points such as the second chart above indicates a stable process, so you know that it is working.
Use the same approach for other steps in embedding frailty identification.
Key challenges
Convincing people that there is a problem
Use hard data to demonstrate the extent of the problem and patient stories and voices to secure emotional engagement. Use peer-led debate and discussion.
Convincing people that the solution chosen is the right one
Come prepared with clear facts and figures, have convincing measures of impact, and be able to demonstrate the advantages of your solution. Involve respected senior figures.
Resources: The NHS Change Model
First steps towards quality improvement: A simple guide to improving services is a resource providing a short overview with the most relevant tools and other resources. http://www.nhsiq.nhs.uk/media/2591385/siguide.pdf
Measurement for Improvement http://www.nhsiq.nhs.uk/media/2594838/ilg_-_measurement_for_improvement.pdf
Other Resources
Measurement for improvement
NHS Scotland Quality Improvement Hub introduction to run charts: http://www.qihub.scot.nhs.uk/knowledge-centre/quality-improvement-tools/run-chart.aspx
1000 Lives Plus Wales How to Improve guide: http://www.1000livesplus.wales.nhs.uk/sitesplus/documents/1011/T4I%20%281%29%20How%20to%20%20Improve%20%28Feb%202011%29%20Web.pdf
The One Hour Improvement Expert: How to Become an Improvement Measure Expert in 60 Minutes [This is a presentation plus transcript]
The A to Z of measurement http://www.nhsiq.nhs.uk/media/2581374/a-z_measurement_glossary_q9.pdf
The run chart: a simple analytical tool for learning from variation in healthcare processes, 2011. http://qualitysafety.bmj.com/content/20/1/46.abstract