Silver Book II was written to address the care needs of older people, specifically older people living with frailty, during the first 72 hours of an urgent care episode. This chapter, edited by Finbarr Martin, Simon Conroy and Bianca Buurman, covers the assessment of older people in an urgent care situation.

Overview
More and more, older people are the major patient group in the context of urgent care scenarios, whether in the acute hospital or in the community. Many older patients living with frailty suffer from a complex combination of multiple diseases, often combining mental, physical and social impairments, yet services are often not designed with these complex needs in mind.
- A quick overall review of the complexity of the case (using for example the Clinical Frailty Scale45), taking into account the medical and psychosocial history, vital signs and symptoms
- Shared goal setting fitting the urgency and the stage of life (i.e. aiming for cure or recovery vs. palliative or end of life care
- Determine the approach and interventions that can serve this goal
- Shared decision making to generate a management plan that best fits the individualised personal goal and has the best balance of added value versus risks and burden
- Reflection on action, to assess the benefit, and to learn together as acute care team.
Principles into practice
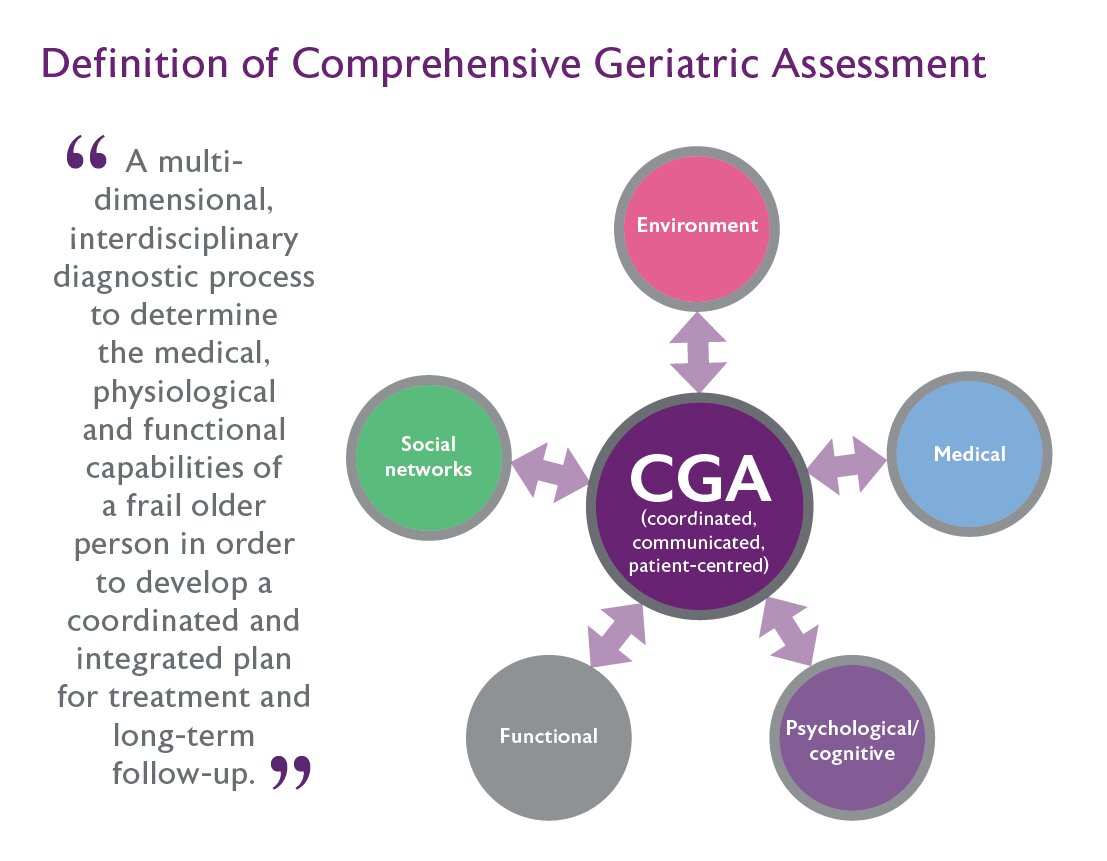
CGA (see Figure 2) is a well evidenced model of care for older people with acute care needs.44,46-56
‘Multidimensional’ - highlights the importance of taking a holistic overview. In this cohort of patients, it is not sufficient to focus simply on one domain or the main problem of the patient. It is the integrated assessment of all of the domains of CGA that allows an accurate problem list to be generated.
‘Interdisciplinary diagnostic process’ – in a mature service, the hierarchy should be flattened such that all staff should feel empowered to constructively challenge within and without of their particular area of expertise.
That this assessment is a process and not a discrete event is also key; the process should continue in an iterative manner over the course of the stay and the diagnostic elements should be sensitive to deviations from the anticipated pathway.
‘Coordinated and integrated plan for treatment’ – reinforces that the team caring for an individual need to know and respect each other’s roles and know and understand what each is doing, and how the medical treatment will impact upon the rehabilitation goals and vice versa. For example, whilst therapists would not need to know the detailed intricacies of the management of acute heart failure, it is important that they know that intravenous diuretics might be required for the first few days that will result in polyuria, and then be able to incorporate continence needs into the rehabilitation plan. Equally, doctors will need to appreciate that just because a patient has grade 5 power on the MRC grading system that does not necessarily translate into useful functional ability.
‘Follow-up’ – as many older people will have multiple long–term conditions, they will usually require some form of on-going care and support. For example, a two-week admission during which Parkinson’s disease medications are carefully titrated and optimised in conjunction with the multidisciplinary rehabilitation process can easily be reversed if there is no on-going titration of L-Dopa once the patient returns home.
|
Resources: Comprehensive Geriatric Assessment
|
Holistic care for urgent scenarios in different settings
Proactive care for older people
Early identification of older people with frailty living at home and providing optimal care to this population has become a high priority58 since being able to maintain functioning and independence is an important goal of older people.59
However, providing optimal care for this population with complex care needs is a major challenge in primary care.60 The current approach is reactive, resulting in unnecessary disease burden, increased after-hours consultations and Emergency Department (ED) visits, and high health care expenditure. Furthermore, most care does not adequately meet the needs of older patients, resulting in an unnecessary loss of physical function and suboptimal quality of life.61 To prevent unnecessary crises, frailty should be identified early and responded to proactively.
Over the past few decades, strategies for early identification and management of frailty have progressed substantially.6,58 Key components of this transformation are the identification of at-risk patients, followed by proactive person-centred care tailored to each patient’s needs.62
These proactive care programs are considered as complex interventions,63 consisting of various (interacting) components:64
- Early identification of those who are at risk
- A frailty assessment among those who are at risk
- A multi-factorial assessment in community-dwelling older people
- A tailor-made care plan
- Care coordination and follow-up.
Several proactive integrated care programmes have been developed and evaluated during the last decade.64,65 However, despite the positive qualitative results among older people and healthcare professionals,66 there is a shortage of quantitative evidence to support these strategies. While some have been shown to preserve function at one-year follow-up,64 others have shown limited or no impact upon function, quality of life or adverse events.65 More effort is needed to develop effective strategies and to determine whether they are feasible and cost-effective. Furthermore, much effort is needed to develop and evaluate high quality interventions in clinical practice that are targeted to the individual needs.67
|
Resources: Proactive care for older people living with frailty
|
Hospital at Home
Hospital at Home (HaH) provides acute hospital-level care in a patient’s home as an alternative to traditional inpatient hospital care.
-
Substitution, also known as ‘admission avoidance’ HaH, where the patient avoids the traditional inpatient environment entirely and usually go from the Emergency Department directly home; and
- Early-discharge HaH, where patients who were admitted to the acute care hospital and who still need ongoing hospital-level care are taken home to complete their hospital stay.
Admission avoidance HaH cares for patients who would otherwise be admitted to hospital. The definition of what constitutes the clinical threshold for hospital admission may vary in different health systems. However, substitution HaH models around the world commonly provide physician and nursing services in the home (in-person or virtual), diagnostic modalities such as blood tests, basic radiography and ultrasound/echocardiography, oxygen or other respiratory therapies, and intravenous medications and fluids. The development of telehealth technology will likely help HaH take on sicker patients over time.
A 2016 systematic review of substitution HaH found results favourable to HaH compared with usual hospital care in terms of reduction in mortality at 6 months (RR 0.77, 95% CI 0.60, 0.99), lower risk of residential care at 6 months (RR 0.35, 95% CI 0.22, 0.57), better satisfaction of care and lower costs.68 A 2017 systematic review of early discharge HaH found that for people admitted for medical conditions, no differences in mortality at 6 months or hospital readmission rates (except for people with COPD).69 There was a reduction in risk of living in an institution setting (RR 0.69, 95% CI 0.48, 0.99) and patient satisfaction with care was better for HaH. A systematic review of HaH that included both substitution and early discharge models on the theory that substituting care in the home for care in the hospital was key to success of the model found lower 6-month mortality in HaH [(OR 0.81, 95% Ci 0.69, 0.95), number need to treat 50], lower readmission rates (OR 0.75, 95% CI 0.59, 0.95), better patient and carer satisfaction with care and lower costs of care.70 Systematic reviews of HaH for specific conditions such as end of life care, heart failure and COPD have been reported with results favorable to HaH.71-73 When implemented at scale (e.g. Victoria state, Australia), HaH can help avoid the need to build new hospitals.
HaH provides better health outcomes, but this is not automatic; it requires a well-coordinated multi-disciplinary service to deliver the right care, at the right time, in the right place - home! HaH straddles the boundary between the hospital and the community, so to deliver excellent HaH care you need staff with expertise and experience in both areas, as well as relationships with the health care professionals in both domains. This enables the team to:
- Speak to the right person when they need to
- Be in the hospital assessing patients, or arranging readmissions when necessary; and
- Provide a seamless transfer of care into the community at all levels of illness and disability.
HaH staff need to be able to work independently. Although telehealth facilities can mean advice and support is closer than ever, staff need to be comfortable going into strangers’ homes and working in their 'territory', without a Nursing Unit Manager or doctor at the end of the corridor. The care must be evidence-based with excellence standardised by utilising clinical pathways and care plans. This includes planning for post-HaH care. It is often necessary to think about how the patients’ non-clinical needs are met, such as whether they have food and other necessary supplies at home, and working out which family or friends can help.
Because the care is in the patient’s home, the patient, their relatives and carers are much more active partners in the care delivery, than when in a hospital ward. HaH teams need to educate patients and their carers about the illness and treatment, and respect the patients’ way of life, while simultaneously maintaining standards to preserve staff safety (for example, requesting that pets are shut in a different room, as sometimes they react badly to a stranger touching their owner; and if applicable, firearms and other weapons are locked away).
Care in the community is always shared care with the general practitioner/family physician and other involved community services. Good relations and communications with these professionals will prevent many problems and improve outcomes. The HaH team must also be adequately resourced to be able to take on patients immediately upon referral, domiciliary care substituting for in-hospital care cannot be provided at the end of a waiting list.
|
Resources: Hospital at Home
|
Pre-hospital
Emergency Medical Services (EMS) provide assessment, ongoing care and transfer to emergency care facilities for older people with illness and injuries.
Simply stated there are two broad models of EMS care with distinct features – the Franco-German and the Anglo-American models.74 Most international systems comprise components from each model.
The Anglo-American (A-A) model is based on the principles of ‘scoop and run’ and the ‘patient is brought to the doctor’ whereas the Franco-German (F-G) is more about ‘stay and play’ where ‘the doctor is brought to the patient’.
The F-G model uses prehospital emergency physicians within paramedic teams in providing advanced assessment and care as if they were a microcosm of a larger healthcare system. More people can be treated on scene and subsequently bypass Emergency Departments into specialty units for continuing care; this is believed to be more cost-effective.
The A-A model on the contrary depends on paramedics delivering assessment and care, sometimes with remote medical oversight. They are responsible for direct transport to Emergency Departments for further assessment and management.
These systems vary distinctly for non-life-threatening conditions and can offer strengths and weaknesses in prehospital geriatric care. The UK’s new Emergency Care Practitioner model could represent a potential hybrid of approaches.75
Management of older people in the pre-hospital setting needs special consideration when it comes to specific conditions, relating to altered anatomy and physiology and the ethical considerations of abuse and futility.
It is increasingly evident that frailty is an important consideration in older people, but there is little research in this area, except for in certain frailty syndromes including falls.76 A small study concluded it was feasible to complete a mini Comprehensive Geriatric Assessment (CGA) to assess the frailty state as part of the prehospital EMS assessment.77 Frailty appears to be a predictor of adverse outcomes including in the pre-hospital setting78 but there is great variation in how it is measured and described. There may be support from paramedics to use frailty assessment tools.79
There is evidence from pre-hospital falls management in older people that specific interventions can affect outcomes. A randomised controlled trial (RCT) looked at clinical protocols as an enhanced offering within the A-A model that reduced emergency ambulance calls for patients attended for a fall.80 However, a systematic review of prehospital EMS services screening and referral to reduce falls failed to identify any ‘high-quality evidence that demonstrates that prehospital services reduce falls in community-dwelling older adults.’81
The increasing awareness of falls being a mechanism for major trauma in older people has recently been highlighted, as have the missed opportunities in the identification and provision of appropriate care. The impact of frailty in trauma outcomes is still being studied, although initial small studies reveal misconceptions around quality of life.82 Provision of early CGA, and geriatricians, may well need to part of future trauma care systems.83
It may be that the F-G system of care offers opportunities to test out extended geriatric assessment in the pre-hospital setting in patients’ natural environments, more so that the A-A model.
Hospital Wide CGA
Frail and multimorbid older people are major users of most hospital services, not just geriatric care.
When these patients are admitted or assessed in non-geriatric services they are usually referred for single disease problems, but diagnosis, treatment and outcomes are heavily influenced by frailty and multimorbidity.
For older people with acute illness, irrespective of the type of the health problem, outcomes (survival, function and prevention of institutionalisation) are better when CGA is performed.44
The first action to be made is to select patients who can benefit from CGA, generally considered to be frail and/or multimorbid older people. Then the challenge is how CGA can be implemented and practised in non-geriatric hospital services. There are different models available; liaison where a geriatrician and a nurse specialist (or Allied Health Professional) visit the patient, nurse-led services, and non-geriatric staff performing CGA.
To provide CGA in non-geriatric services, these components are needed:
- Routines and tools for selection of patients who can benefit from CGA
- Routines for a systematic and structured assessment based on CGA
- Competence available: doctors, nurses, physiotherapists and occupational therapist with special competence in older people
- Enough time to perform the assessment and develop a realistic care plan, also to be followed after discharge from hospital.
Follow-up is crucial as CGA will usually generate several issues that are important to address, but not necessarily requiring immediate management the acute hospital. Communicating such issues to the ongoing care provider is one means of trying to maintain independence in the community and reduce readmissions.
CGA remains the gold standard approach to improving a range of outcomes for frail and multimorbid older people in acute hospitals. Unit-based services are recommended over liaison services.44,49 A toolkit for implementation of CGA in acute services is available here. Such toolkits aimed at enhancing the delivery of CGA by non-specialists can be useful but require prolonged geriatrician support and implementation phases, and sustainability without geriatrician input is uncertain.36
The emergency department (including geriatric emergency medicine)
The emergency department is frequently a chaotic, time-constrained setting in which to provide complex care for common geriatric problems such as safe mobilisation, cognitive impairment, polypharmacy, and frailty.
Nonetheless, emergency medicine and geriatrics society endorsed consensus-based guidelines exist highlighting protocols, training, and quality improvement metrics required to optimise the outcomes from emergency care.84 Two features are essential for effective geriatric emergency care:
- Transdisciplinary team-based philosophy extending beyond the emergency department
- Holistic approach that incorporates unique patient priorities within the context of the acute medical problem (see Figure 4)
A transdisciplinary philosophy of geriatric emergency medicine requires coordination of services beginning in the pre-hospital setting and extending through the emergency department to inpatient services and outpatient referrals. Access to baseline functional and cognitive status, co-morbid disease burden, current prescriptions and recent changes to medications, social support mechanisms, and advanced directives permit the emergency department to distinguish acute from chronic illness/injury, while aligning the diagnostic and therapeutic approach with patient’s goals of care.
In North America, emergency medicine has described core competencies for geriatrics,86 while in Europe a curriculum has been published.87 Internationally, minimum geriatric emergency care standards also exist.88 Optimal geriatric emergency care includes adapting age-related principles into diagnostic and therapeutic decision-making, establishing protocols to identify and manage cognitive dysfunction, polypharmacy, unsafe ambulation, and vulnerability.89 Free online resources, including blogs, podcasts, published reviews, and interactive educational modules exist to learn more about these principles (see box below).
|
Resources: Geriatric Emergency Medicine
|
One ongoing challenge is the evidence upon which geriatric emergency care recommendations are built. For example, existing instruments identify cohorts but not individuals at high-risk for vulnerability/frailty,90 dementia91 or falls.92 On the other hand, emergency medicine has ample evidence to guide delirium detection.93 Once accurate frailty screening instruments exist, the next challenge is linking higher risk patients to effective interventions. Even the most common frailty syndromes like delirium and falls prevention lack high-quality evidence (randomised controlled trials in ED settings) upon which to build protocols.94 Furthermore, lower quality evidence frequently relies on resources not readily available in every ED.
- Although geriatric emergency department guidelines and quality indicators provide specific recommendations regarding the infrastructural elements of an age-friendly department (including added comfort of reclining chairs, extra thick gurneys/trolley matresses, visual orientation cues associated with lightening and wall colouring, and acoustic enhancements to minimise disorienting noise pollution), these components are less important than the staff training and geriatric protocols.84,95
- Frailty-centric protocols developed in collaboration with transdisciplinary teams should include screening for falls, cognitive dysfunction, medication safety, elder abuse, functional status, and frailty.84
- Screening protocols should be linked with actionable responses. For example, when possible cognitive impairment is identified reliable healthcare partner/family should be engaged to determine accuracy of the presenting complaints and communicate post-emergency department care recommendations.96
- Atypical presentations of common diseases should be anticipated to avoid anchoring bias and premature closure.97 For example, Urinary Tract Infection (UTI) is frequently assumed in the setting of delirium with associated pyuria but delirium is an inaccurate diagnostic predictor of UTI.98
- Observation Units or Frailty Units provide a structured, less chaotic setting for multidisciplinary geriatric assessments to reduce emergency department returns and admission rates.99,100
- Frail older adults frequently rely upon healthcare partners (spouse, family, or neighbour), so disposition and post-ED management decisions must often consider the availability and resources of these caregivers.96,101
The emergency department is often the first available healthcare resource for older adults during times of acute illness or injury. As the front door to the hospital, emergency medicine must contribute to system-level adaptations for aging populations and can accelerate positive change when engaged. Existing geriatric emergency medicine curricula, guidelines, and quality metrics provide a foundation upon which emergency departments worldwide can align care delivery with best evidence resources. In addition, the emergency medicine path to ‘geriatricise’ training, infrastructure, and protocols could also guide other specialties’ approaches to catalyse older adult acute care.
Acute Medical Unit
The interface between community and hospital offers unique opportunities for frailty screening, early management and appropriate onward referral.
Older adults are frequent and increasing users of the AMU. Early, frailty-attuned care can improve outcomes, but to deliver this will necessitate changes in systems and infrastructures. Multidisciplinary assessment and management (CGA)44 of older adults with frailty reduces functional decline and institutionalisation. While CGA is usually delivered by specialist teams, the process can, and should, begin in the AMU. Assessing physical, mental and social functioning to offer patient-centred care is a core skill for the AMU.
Staffing - Best practice is driven by role modelling. A senior member of AMU staff should be designated a frailty champion. This person does not need to be a trained geriatrician, but availability and visibility of geriatric specialists within the AMU is essential. Optimal care of the older adult requires multidisciplinary expertise. Having specialist nurses and allied health professionals embedded within the AMU team is preferable to liaison services. There also needs to be easy and prompt access to other disciplines including speech and language, dieticians and social work.
Training - Delivering older-person-attuned, holistic care is challenging and may not be familiar to AMU staff. National and regional training bodies need to ensure core competencies in frailty. At local level, there should be ongoing, in-service training relevant to older adult care. This should be complemented by rolling programmes of quality improvement specific to older adult needs.
Infrastructure - The physical infrastructure of the AMU needs to promote independence and safety of patients with physical or cognitive impairments. A designated area for older adults with frailty will help. There should be access to equipment, toileting and other aids required for people with varying levels of dependence. Time critical medications (e.g. for Parkinson’s disease) and equipment (e.g. replacement PEG tube) need to be easily accessible.
Identification - Although various methods exist to assess for frailty, perhaps the most widely used (and best validated in the acute context) is the Clinical Frailty Scale. AMUs need to implement a system that identifies older adults that would benefit from the CGA approach. Once frailty is identified, specific assessment tools are available to identify medical, cognitive, social and functional needs. These should be incorporated into a clerking proforma.
Information - Older adults are often living with complex comorbidity, polypharmacy and disability. AMUs should have access to relevant background information on a person’s usual health, function and healthcare wishes. Early, comprehensive medicines reconciliation is mandatory, including identification of ‘high risk’ medications that may require review during a period of illness. On discharge from AMU, systems should allow information to be shared with primary care or the subsequent clinical team. The initial AMU assessment should establish the person’s priorities and goals, where relevant obtaining documents such as welfare guardian powers or advanced care plans.
Pathways - In the context of frailty, illness tends to present in stereotyped ways. AMUs should have standardised operating procedures for management of the common older age syndromes (falls, delirium, suspected neglect). Protocols that limit potentially harmful interventions such as urinary catheters and sedation are also useful. Planning for safe discharge begins in the AMU. Effective transition between teams is dependent upon integration of the AMU with primary care, specialist older adult services and social care. Availability of community services allows for early discharge of appropriate patients for ongoing CGA. AMU staff should know the local services available and how to access them.102
Orthogeriatrics
Hip fracture is a major public health problem, with high incidence rates in older people worldwide.
Orthogeriatric care is an adaption of Comprehensive Geriatric Assessment,106 and is effective when it is targeted at an older, frail, multi-morbid cohort at risk of future falls and/or fractures at a high risk of perioperative complications such as delirium, pneumonia, pressure sores and malnutrition. Orthogeriatric co-management has been shown to be the most effective model of care to manage older patients hospitalised with hip fractures. This interprofessional multidisciplinary model of care is best placed to address the complex hip fracture healthcare needs and has been shown to deliver improved outcomes across several clinical and cost-related measures - decreased time to surgery, shorter length of stay, improved postoperative clinical outcomes, decreased mortality, and lower cost.107,108
Different ways of delivering orthogeriatric care have been described based on the level of medical involvement in patient care.109 However, the most integrated model of co-management between the medical physician and surgical team has demonstrated the best outcomes.107-109
An orthogeriatric service needs to consider the entire journey of hip fracture care, from presentation to the Emergency Department all the way through to rehabilitation and recovery. All hospitals and trauma units operate differently - there is no universally agreed way of delivering an orthogeriatric service and local adaptation is required. Hence, the initial step in developing an orthogeriatric service is to understand the local hip fracture pathway. A mapping exercise of the patient journey is crucial to understand the current provision of care. Mapping allows further identification of respective members of the interprofessional multidisciplinary team and from there, identification of ‘clinical champions’ from each profession. These clinical champions should come together to form a formal stakeholder group, who will be able to analyse the mapped patient pathway, identify gaps in the service and the changes required to deliver the optimal hip fracture pathway.
The UK NICE guidelines provide an interactive patient pathway defining the optimal patient pathway. An extensive list of further resources is available at the UK National Hip Fracture Database website, which includes referenced publications, business case templates and other useful links.
The aim of a business case is to persuade those in charge of finances and service provision that the orthogeriatric service is in the best clinical interest of the patients and, perhaps more importantly, in the best financial interest of the hospital. It is a short document that will take the recipient on a journey from conception of the idea to delivery of the service. When the business case has been approved by the hospital management, which may include executive and non-executive members, managers, clinicians, and financial representatives, the service may be started as a small pilot, followed by constant evaluation of the service and quality improvement work, led by the core clinical champions steering group. The Plan, Do, Study, Act (PDSA) cycle, is a widely accepted and used framework for developing, testing and implementing change.
The role of patient or public advocates can be a powerful tool in delivering the message of orthogeriatric care and also needs to be encouraged. This can be locally through patient support groups and national bodies via established osteoporosis patient organisations. In addition many national societies, for example the orthopaedic and geriatric medicine societies have adopted orthogeriatric co-management. These societies have come together to support the work of the Fragility Fracture Network and more recently its Global Call to Action.110 Hence, a way of sustaining an orthogeriatric service is by aligning local initiatives to a much larger national/ international initiatives.
Peri-operative care for older people
Older people aged 65 years and older account for a considerable proportion of those undergoing emergency surgery.
This older cohort frequently displays age-related physiological impairments, multimorbidity and geriatric syndromes such as frailty, sarcopaenia, functional and cognitive impairment. Across emergency surgical populations, frailty in particular is associated with higher rates of postoperative mortality, morbidity, functional decline and a prolonged length of hospital stay.111 Furthermore, outcomes are also poor although less well described in emergency surgical patients managed non-operatively.
There is a growing movement to identify frailty and respond to it using holistic assessment and management. For example, in the United Kingdom it is suggested all patients aged over 65 years, admitted under general surgery, be screened for frailty using the Clinical Frailty Scale. The identification of moderate or severe frailty should trigger Comprehensive Geriatric Assessment (CGA) delivered by a geriatrician led multidisciplinary team. In addition, preoperative CGA should be considered for patients admitted under surgical teams with multimorbidity, cognitive impairment, functional dependency and in whom there is difficulty in deciding whether surgery should be undertaken. This should prompt shared decision-making, advance care planning and proactive rehabilitation and discharge arrangements.
Provision of perioperative services are growing and illustrative case studies are described by Centre for Perioperative Care. In keeping with the emerging evidence base, services should be underpinned by geriatrician led and multidisciplinary delivered CGA.
Key points:
- At-risk patients admitted under surgical teams should be screened for frailty
- CGA based services should be available for older surgical patients
- Integrated perioperative pathways should involve geriatricians, surgeons and anaesthetists working with the multidisciplinary team
- Improving quality in perioperative eservices across surgical specialties requires use of a national minimum dataset (e.g. National Emergency Laparotomy Audit)
Oncogeriatrics
As increasing age is the most important risk factor for developing cancer, the majority of patients with cancer are older than 65 years.
Cancer treatment is evolving rapidly, and newer treatments such as immunotherapy may be tolerated even in older patients. Due to the constant development in oncology, one of the most important issues in oncogeriatrics is to seek collaboration with medical oncologists, cancer surgeons and radiation oncologists before making treatment decisions in older people with frailty and cancer. On the other hand, most of the clinical cancer trials have been performed in younger cohorts or in selected older patients, which means each case needs to be evaluated individually taking into account patient goals and preferences and frailty.112
There are consistent recommendations internationally to perform Comprehensive Geriatric Assessment (CGA) in older patients with cancer to uncover impairments not captured through a routine examination,113,114 Following GA, cancer patients can be classified according to their degree of frailty, remaining life-expectancy can be estimated and the risks vs benefits of treatment can be considered in detail.115,116 Furthermore, geriatric co-management may optimise the patient before treatment and during the treatment trajectory. An example is pre-habilitation before cancer surgery, which aims to increase the patient's functional reserves preoperatively.117 Optimisation may consist of dealing with comorbidities and polypharmacy, nutritional support, physical exercise, social support, and handling treatment complications. In people with cognitive impairment, the need for support during decision-making and treatment delivery is particularly central due to risk of poor compliance with complicated regimens, delirium during treatment and further cognitive decline.
In some countries, all older adults with cancer undergo screening to identify patients in need of a GA. A screening tool specifically developed for cancer patients is the Geriatric-8 (G8).118,119 In order to detect cognitive impairment and poor mobility, G8 may be supplemented with mini-Cog and an objective performance measure such as gait speed.
Resources: Oncogeriatrics
|
Cardiogeriatrics
Cardiovascular symptoms, including chest pain or discomfort, shortness of breath, palpitations, and dizziness/syncope, are among the most common reasons for older adults to present for urgent evaluation.
Key elements of initial assessment include problem identification (recognising that non-specific presentations are common and that multiple problems frequently co-exist), risk stratification, and attending to urgent issues (considering overall prognosis apart from the primary cardiac issue). This is followed by additional testing, if indicated, incorporating patient priorities into the decision-making process.
In general, management of older adults with urgent cardiovascular conditions should be in accordance with pertinent guidelines in conjunction with the patient’s broader health status, goals of care, and personal preferences. Thus, to the extent feasible, shared decision-making should be employed in determining care intensity, with due consideration given to the potential risks and benefits associated with various management options.
Key questions that may need to be addressed in the urgent setting include
- Whether the patient desires cardiopulmonary resuscitation in the event of cardiac or respiratory arrest
- Whether the patient desires invasive procedures (if indicated) such as cardiac catheterisation, percutaneous coronary intervention, or cardiac surgery
- Whether the patient desires admission to the intensive care unit and treatment with intravenous inotropic and vasopressor medications if needed to support the heart and circulation.
In situations where the patient is unable to actively participate in decision-making due to illness severity, cognitive impairment, or acute stress, a surrogate decision-maker, such as a designated durable power of attorney for health care, should act on the patient’s behalf.
Key points:
- Cardiovascular conditions are highly prevalent and are among the most common reasons for older adults to seek urgent medical attention.
- Symptoms and physical findings are often atypical, so it is important to keep an open mind and to consider a broad differential diagnosis of both cardiac and non-cardiac disorders.
- A focused history and physical examination are critically important for narrowing the differential diagnosis and determining the likelihood of a serious or life-threatening cardiac or non-cardiac condition.
- Cardiology consultation should be considered as needed to assist with management, especially in cases where a life-threatening condition is suspected.
- Optimal management of older adults with acute cardiac conditions involves integrating pertinent guideline recommendations with each unique patient’s personal preferences using a process of shared decision-making.
- If the patient is unable or does not want to make difficult health decisions, it is essential to incorporate pre-existing advance directives and surrogate decision makers to ensure that the patient’s stated wishes are honoured.
Transitional care
Many older adults experience adverse health outcomes in the first months after hospitalisation: 15-20% are readmitted within 30-days, and three months post-discharge, 20-30% experience functional decline or have died.
Transitional care was initially set up to reduce readmissions after hospitalisation and Mary Naylor122 and Eric Coleman123 are founders of the care model. It is different from case management models, as transitional care is considered as a time-limited service, provided up until six months post-discharge. The model is also distinct from disease management as the approach is more holistic, but can include disease-specific symptom management. The first studies were conducted with heart failure patients, but the model further developed also to serve older people with frailty.
The model consists of:
- Comprehensive assessment, including assessment of risks
- Education around medication, symptoms and what to do in case of problems
- Patient and family engagement
- Warm handover between hospital-based team and primary care team, ensuring that information is directly handed over to the right persons, patients are seen, and questions can be asked
- Nurse care coordination during and after discharge
- A visit shortly after hospital including medication reconciliation
- Follow-up of care in the home situation.
There is a huge body of evidence that supports the effectiveness of the model.124-126 It reduces readmissions and mortality in many patient groups, but meta-analyses also demonstrate that the intervention needs to be intensive enough, including a visit shortly after discharge. This is needed, as often readmissions occur in the first two weeks post-discharge.127
The transitional care model has been linked to the CGA-consultation model128 and has been successfully applied in the Emergency Department setting leading to lower rates of admissions and admission days.129
Community hospitals
Locality-based hospitals have featured worldwide for many years, although not all are called community hospitals and different models exist; for example Finland refers to ‘Health Centre Hospitals’.
Medical models of care differ from country to country and hospital to hospital with some having daily local General Practitioner input, with out of hours cover in the evenings and weekends. Others have Advanced Nurse Practitioners responsible for the provision of daily care, with less frequent specialist support. Many such hospitals have arisen when local acute hospitals have closed down.130
With increasing complexity and frailty, there is a need for geriatric competencies throughout the locality hospital workforce. Staff need to be able to apply CGA. Wherever these hospitals exist in the world and whatever the local provision, there will be a requirement for staff to deliver the care against the CGA derived plan.
Specific competencies that locality hospital teams need to be able to evidence include:
- Care planning and goal setting (including Advance Care Plans)
- Documentation of the care plan which is as robust as in acute care, and a daily record and update should be recorded for every patient
- Knowing how, where and when to access specialist help
- Staff skilled in recognising the subtle signs of deterioration in older people, and as the community hospital may not have the full resources available to them it is essential that staff are vigilant in recognising and responding effectively, in order to prevent an emergency situation
- Pathways to urgent care (if and when needed) which are clearly identified
- Investigations conducted in a timely manner and not viewed as if the individual was in their own home, and offered on a same-day basis if there is an urgent care need
- Liaison with old age psychiatry for people with complex psychiatric conditions should be available and timely
- An environment conducive to those with dementia with support e.g. meaningful activities
Service configuration and delivery will vary from locality to locality, but the core approaches above should be universally available. Locality hospital staff need to have ongoing learning opportunities and case review of patients under their care.
Many locality hospitals have both ‘step up’ and ‘step down’ functions, acting as proactive dynamic, community centres. Models in which the communities are engaged in shaping the delivery of local services should be encouraged, so the local community feels connected and engaged with the locality hospital.
Care homes
Older people who reside in Nursing Homes (NHs) are frequently transferred to acute care hospitals.
In order to manage acute changes in condition in the NH as an alternative to transfer to an ED, the infrastructure and incentives must be aligned with this goal. Infrastructure includes:
- Adequate numbers and training of nursing staff
- Availability of physicians and advanced practice clinicians (e.g. nurse practitioners and physician associates or assistants) either on site, via telephone or telemedicine
- Availability in a reasonable time frame of laboratory testing, imaging services, oxygen, and medications and fluids, including oral and parenteral/intravenous administration.
Incentives include both financial and regulatory. Reimbursement for care must reward avoiding ED visits and hospitalisation. In some countries, acute care hospitals incur financial penalties for high rates of 30-day readmissions, and NH quality measures include rates of 30-day hospital readmissions and returns to the ED without admission. NHs should not incur regulatory of financial penalties when using evidence-based and expert-recommended care protocols to manage acute changes in condition in efforts to reduce unnecessary hospital transfers.
In addition to infrastructure and incentives, effective implementation of programs requires substantial effort on the part of NHs. Facility leadership, including the administrator, director of nursing, and medical director, must support programs designed to manage acute changes in condition in the NH whenever safe and feasible. If the NH is part of a corporate chain, corporate leadership must also support the program implementation. The program should be incorporated into everyday care routines and be a component of the facility’s quality improvement activities. Electronic Health Records (EHRs) are increasingly being used for clinical documentation in NHs; incorporation of key tools into the clinical workflow within the EHR is another strategy that may enhance the effectiveness of these programs.
Several strategies are critical to effectively managing acute changes in condition in NHs, including:
- Identifying changes in condition early before they become severe enough to require hospitalisation (e.g. infection, dehydration)
- Managing some changes in condition without transfer when safe, feasible, and consistent with resident/patient care preference (e.g. cough and low grade fever, shortness of breath with adequate oxygen saturation, altered mental status and/or behavioural changes)
- Improving communication and documentation practices within NHs and between NHs and hospitals (e.g. using the SBAR method of communication and standardised, critical data elements in transfer forms)
- Using comfort or palliative care when the risks of hospitalisation outweigh the benefits, and is consistent with resident/patient/family preferences (e.g. recurrent aspiration in a resident with end-stage dementia).
Several such tools and programs are now available that incorporate these strategies (see below).
|
Resources: Safe and feasible urgent care in the nursing home
|



{kind=link}
{kind=link}
{kind=link}